Arrhythmias by type re entry. The occurrence of arrhythmia according to the mechanism: early and late postdepolarization, macro- and micro-re-entry
An excitatory impulse is formed on the cell membrane by generating an action potential. Depolarization of one cell causes a decrease in the negative resting potential of the neighboring cell, as a result of which it reaches the threshold value, and depolarization occurs. The shape, orientation, and presence of gap junctions between myocardial cells cause an instantaneous transmission of depolarization, which can be described as a wave of depolarization. After depolarization, the cell cannot depolarize again until a certain amount of time has passed for the cell to recover, the so-called refractory period. Cells that are able to depolarize are called excitable, and those that are unable are called refractory.
In sinus rhythm, the source of excitation waves is the sinus node, between the atrium and ventricle they are transmitted through the atrioventricular node. Impulse generation (and heart rate) is regulated by the autonomic nervous system and circulating catecholamines. With tachyarrhythmia, this regulation is disturbed, and, as a result, the heart rhythm is disturbed.
Blockade of the
Electric waves will propagate as long as there are excitable cells in their path. Anatomical obstructions such as the annulus of the mitral valve, vena cava, aorta, etc. do not contain cardiomyocytes and therefore prevent wave propagation. This phenomenon is called a permanent blockade of conduction, since this blockade is always present. Another important source of a fixed blockade of conduction is dead cells, for example, at the site of a scar after myocardial infarction.
When the blockade is present only under certain circumstances, one speaks of a functional blockade of conduction. An example is ischemia, in which myocardial cells are damaged and lose their ability to conduct excitation. It is the functional block that prevents the reverse propagation of the wave, since the cells located behind the propagating wave of excitation are temporarily refractory and do not pass the excitation retrograde. Other causes of functional blockade are cyanosis, myocardial distension, frequency or direction of the wave.
Mechanism of development of arrhythmia
There are 3 independent mechanisms:
- Increasing automatism.
- Re-entry (mechanism of "re-entry" of the excitation wave).
- trigger activity.
Mechanisms of arrhythmias
Increasing automatism
If a group of myocardial cells depolarize faster than the sinus node, they will act as a source of excitation waves conducted throughout the myocardium. This focus can be located both in the atria and in the ventricles. If it is in the atrium, it suppresses the sinus node. Since the cells are usually localized in one place, tachycardia is called focal. Locations where cardiomyocytes are most likely to change size/shape or act high pressure, include areas where the veins (superior vena cava, pulmonary) flow into the atria, terminal crest, coronary sinus, atrioventricular node area, mitral and tricuspid valve ring, ventricular outflow tract.
Re-entry mechanism ("re-entry" of the excitation wave)
It accounts for more than 75% of clinical forms of arrhythmias. The reason is the uncontrolled propagation of an excitation wave against the background of an excitable myocardium. For the development of re-entry (reciprocal) tachycardia, there must be at least 2 pathways around the area of impaired conduction. The best example is VT due to pulse recirculation around a scar in the left ventricle.
- Scar tissue is the site of the blockade, around which normal impulses from the sinus node pass to the healthy myocardium (A). Impulses pass slowly through damaged myocardial tissue (B). 2 separate ways of carrying out turn out.
- Immediately following the impulse from the sinus node is a ventricular extrasystole that passes through site A but is blocked in site B, still refractory from the previous sinus contraction.
- However, the distal end of site B is already capable of excitation, and the impulse travels back through site B, whose conduction has already recovered during the period in which the impulse reached the proximal end. In site B, the rate of impulse conduction decreases, while the cells of site A are again able to excite and conduct an impulse.
Thus, a re-entry wave is formed, which is constantly supported by excitation sites in the myocardium.
trigger activity
Combines the features of both of the above mechanisms. Caused by spontaneous (automatic) post-depolarization occurring in phase 3 (early post-depolarization) or phase 2 (late post-depolarization) of the action potential. Such post-depolarizations are often caused by extrasystoles and inductions similar to re-entry tachycardia. When post-depolarization reaches a threshold level, a single or group action potential is formed. Post-depolarization can be caused by ischemia, drugs that prolong the QT interval, cell damage, or low potassium. According to this mechanism, tachycardia of the "pirouette" type and rhythm disturbances due to the toxicity of digoxin develop.
Electrophysiological studies
Most effective in the diagnosis of tachycardia. When the diagnosis is already confirmed or strongly suspected, this procedure is combined with catheter ablation as part of the treatment of an arrhythmia. It should be noted that electrophysiological studies usually measure the length of the cardiac cycle (in ms), and not the heart rate, for example, 60 per minute equals 1000 ms, 100 per minute equals 600 ms, 150 per minute equals 400 ms.
Charting (mapping) the electrical activity of the heart
An electrophysiological study is mistakenly considered a complex procedure. In essence, this is the registration of cardiac impulses, both in sinus rhythm and in arrhythmia, or in response to pacing of various zones of the heart. The ECG contains most of this information, therefore, during electrophysiological studies, an ECG is recorded in 12 leads.
Intracardiac electrography
With an ECG, cardiac activity as a whole is summed up. Data on the electrical activity of a specific area of the heart is obtained by placing 2 mm electrodes directly on the surface of the heart muscle. Intracardiac cardiography is more accurate and gives the best data at a recording rate four times faster than ECG.
A potential difference can be recorded both between two adjacent electrodes (bipolar electrogram), and between one electrode and infinity (unipolar electrogram). A unipolar electrogram is more accurate in terms of the direction and location of electrical activity, but it is also more sensitive to interference. It is important to note that pacing can be performed through any of these electrodes.
Pacing protocols
In an electrophysiological study, pacing is performed in a predetermined manner called programmed pacing. It is of three types:
- Step-increasing pacing (incremental pacing): the interval between stimuli is set
slightly below sinus rhythm and decrease in steps of 10 ms until blockade occurs or a predetermined lower level is reached (usually 300 ms). - Extra stimulus pacing: a chain of 8 stimulations at a fixed interval is followed by an additional (extra stimulus) that is delivered between the last impulse of the leading chain and the first extra stimulus. The impulses of the leading chain are designated S1, the first extra stimulus is S2, the second extra stimulus is S3, etc. An extra stimulus may be given after a perceived heart contraction (additional contraction).
- Burst pacing: pacing at a fixed cyclic rate for a specified time.
The catheter is inserted into the right side of the heart through the femoral veins with fluoroscopic guidance. These right anterior (top) and left anterior (bottom) views show the standard placement of a catheter in the upper right atrium (near the sinus node, at the bundle of His, at the apex of the right ventricle) and a catheter through the axis of the coronary sinus, circumflexing behind left atrium along the atrioventricular sulcus. From this position, an intracardiac electrogram is recorded from the left atrium and ventricle. Catheters are often inserted through the right or left subclavian vein.
In the intracardiac ECG, data are ordered as follows: upper right atrium, bundle of His, coronary sinus, and right ventricle. The readings of each bipolar catheter are lined up from proximal to distal. In sinus rhythm, the onset of excitation is recorded in the upper part of the right atrium, it passes through the bundle of His, and then along the coronary sinus catheter from the proximal to the distal position. Early ventricular excitation is recorded in the apex of the right ventricle (where Purkinje fibers are present).
Indicators of the normal sinus interval: RA - 25-55 ms, AN - 50-105 ms, HV - 35-55 ms, QRS<120 мс, корригированный ОТ <440 мс для мужчин и <460 мс для женщин.
Application of electrophysiological studies
sinus node function
Sinus node function is measured by adjusted sinus node recovery time and sinus conduction. However, these studies are not reliable because sinus node function is affected by autonomic tone, drugs, and testing errors. Sinus node dysfunction is best diagnosed with ambulatory monitoring and exercise testing. An invasive electrophysiological study very rarely allows a final decision to be made regarding the need for implantation of a permanent pacemaker in a patient.
Atrioventricular conduction
Atrioventricular block. The degree of blockade is assessed using an ECG, in addition, you can also set the level of blockade (directly atrioventricular node, or the His-Purkinje system, or blockade below the node). The level of blockade is easily established using an electrophysiological study. With blockade of the atrioventricular node, the time of AN is increased, with subnodal blockade - HV. AN time (but not HV time) can be reduced with exercise, atropine or isoprenaline, and increased with vagal testing.
The function of the atrioventricular node is assessed both antegrade (from the atria to the ventricles) and retrograde (from the ventricles to the atria), using stimulation according to the step-increasing technique and the extrastimulation method. With incremental stimulation of the upper part of the right atrium, conduction is observed at the points of the bundle of His, the apex of the right ventricle before the onset of blockade. The longest pacing interval at which blockade occurs during an antegrade study is called the Wenckebach period (Wenckebach point). The normal value is less than 500 ms, but it can increase with age or under the influence of the tone of the autonomic nervous system. The Wenckebach period is also measured during retrograde examination, but in this case, the absence of ventricular-atrial conduction may be a variant of the norm. At the point of the upper part of the right atrium, extra stimulation is applied. Reducing the interval between S1 and S2, atrioventricular conduction is assessed. The longest interval at which blockade is observed is called the nodal atrioventricular effective refractory period. The indicator is measured at intervals of the leading chain of 600 and 400 ms. In the presence of ventricular-atrial conduction, the retrograde indicator of the effective refractory period of the atrioventricular node is measured.
Conduction attenuation: is the key to the physiological properties of the atrioventricular node. With a decrease in the interval between impulses passed through the atrioventricular node, the speed of conduction through it decreases. On atrioventricular conduction, this manifests itself with a decrease in the interval of atrial stimulation by lengthening the AH interval (AV time). This phenomenon can be observed during incremental and extrastimulation. If you plot the AH interval versus S1S2 (= A1A2) during extrastimulation, you can get an antegrade conduction curve.
Dual physiology of the atrioventricular node: in many patients (but not all) it is possible to determine two electrically) connections between the atrium myocardium, tightly surrounding the atrioventricular node, and the atrioventricular node itself, which have different conduction properties. The slow pathway, unlike the fast pathway, has a lower conduction velocity and a shorter effective refractory period. This is revealed when constructing an antegrade conduction curve. With a longer A1A2 time, the impulse conducts mainly along the fast path, however, when it reaches the point of the effective refractory period, the conduction will go along the slow path, and there will be a sudden lengthening of the AH time. This phenomenon is referred to as AH gap tearing and is characterized by >50 ms lengthening of the AH period after a 10 ms decrease in the A1A2 interval. The presence of dual pathways of the atrioventricular node is a predisposing factor for the development of AVNRT.
Definition of abnormal atrioventricular pathways
Normally, there is only one connection between the atrium and the ventricle. Activation of the atrium (via ventricular pacing) or ventricular (via atrial pacing or in sinus rhythm) must begin at the atrioventricular node. Additional conductive paths must conduct the pulse without attenuation. Their presence can be detected by abnormal modes of activation, as well as by incremental or extra stimulation.
atrial pacing. As the impulse of the atrioventricular node decreases, the activation of the ventricles occurs to a greater extent with the help of accessory pathways. Accordingly, there will be persistent atrioventricular conduction and an increase in the duration of the ORS complex. It is important to note that if the effective refractory period of the accessory pathways is shorter than the effective refractory period of the atrioventricular node, then the QRS complex will narrow sharply and the atrioventricular conduction time will suddenly lengthen when blockade of the accessory pathways occurs.
Ventricular stimulation. The normal order of atrial activation is bundle of His, coronary sinus (proximal to distal), and finally the upper right atrium—this activation pathway is called concentric. If atrial activation occurs along accessory pathways, an eccentric type of activation is observed. The site of early atrial activation will be localized to the accessory pathways, and sustained ventricular-atrial conduction will also be observed.
Arrhythmia induction
The presence of accessory pathways, dual physiology of the atrioventricular node, or a scar in the ventricular wall is a predisposing factor for the development of tachycardia, but this does not mean that it will necessarily occur. Diagnosis can be confirmed by induction of tachycardia.
In addition to the described methods of pacing, stimulation in bursts, extrastimulation with multiple extrastimuli and additional stimuli are used. If it is impossible to induce tachycardia, I repeat all these methods - against the background of the introduction of isoprenaline (1-4 μg / min) or its bolus infusion (1-2 μg). This method is especially good at detecting tachycardias that develop according to the mechanism of increased automatism. Active induction protocols increase the likelihood of unwanted arrhythmias. Like FP or FJ.
When induced tachycardia occurs, the patient's ECG should be compared with their 12-lead ECG recorded earlier at the time of symptom onset.
Programmable ventricular pacing
Electrophysiological studies that aim to induce VT (VT induction study) have previously been used to stratify the risk of sudden cardiac death, assess the effectiveness of antiarrhythmic drugs in suppressing VT, and the need for implantation of an cardioverter-defibrillator. Currently, there is evidence of a small prognostic role of this study, so the decision to implant an cardioverter-defibrillator must be made taking into account other risk factors, in particular left ventricular function. An electrophysiological study may be useful before inserting an artificial pacemaker for other reasons:
- For help programming the device.
- Is VT well tolerated haemodynamically by the patient?
- Is it easily interrupted with overdrive pacing?
- Is there ventricular-atrial conduction? During ventricular pacing or VT?
- To assess the possibility of VT ablation (eg, bundle branch ablation).
- To determine the presence of other rhythm disturbances, including easily caused arrhythmias.
Programmed ventricular pacing is performed using the protocol developed by Wellens, or a modification thereof.
Clinical indications
- Confirmed tachycardia with the presence of clinical symptoms (as the first stage of diagnosis and ablation procedure).
- Risk stratification of sudden cardiac death.
- Suspected but not confirmed tachycardia with clinical symptoms (for diagnostic purposes only).
- Wolff-Parkinson-White syndrome.
- Syncope of unknown origin (presumably related to arrhythmia).
- Suspicion (in rare cases) of intra-atrial or atrioventricular node block (not documented).
Protocol for programmed ventricular pacing
- From the apex of the right ventricle, extra stimulation reduces the interval between pulses until the refractory period is reached:
- 1 extrastimulus during sinus rhythm;
- 2 extrastimuli during sinus rhythm;
- 1 extra stimulus after 8 stimulated contractions at 600 ms;
- 1 extra stimulus after 8 stimulated contractions at 400 ms;
- 2 extrastimuli after 8 stimulated contractions at 400ms;
- 3 extrastimuli during sinus rhythm 0 ms;
- 2 extrastimuli after 8 stimulated contractions at 600ms;
- 3 extrastimuli after 8 stimulated contractions at 400ms.
- If a ventricular arrhythmia cannot be induced, repeat the steps from the right ventricular outflow tract. Thus, the activity of the pacing protocol gradually increases, while the specificity of the procedure decreases. The most valuable result from a diagnostic point of view is the induction of prolonged monomorphic VT by one or two extrastimuli, which indicates a potential risk of developing ventricular arrhythmia. Short-term VT, polymorphic VT, and VF are non-specific findings.
New technologies
Electrophysiological procedures become more and more complex (for example, in AF or CHD) and are accompanied by an increasing radiation exposure to the patient. Both of these problems were solved with a non-fluoroscopic 3D mapping system. A computer-generated image of the cardiac cavity of interest is generated, overlaid with electrical activity and the location of the electrophysiological catheter (Fig. 10-4). In some cases, it is possible to perform an electrophysiological examination and ablation without the use of X-rays. What's more, 3D CT or MRI images of the patient can be imported and used as a guide image.
At the heart of all arrhythmias is a violation of the formation or conduction of an impulse, or a simultaneous disorder of both functions of the conduction system. Arrhythmias such as sinus tachycardia and bradycardia are associated with an increase or decrease in the automatism of the cells of the sinus node, respectively. In the origin of extrasystole and paroxysmal rhythm disturbances, 2 main mechanisms are distinguished: increased automatism of ectopic foci, re-entry of excitation (re-entry) and circular motion of the impulse.
Increased automatism of ectopic foci may be associated with acceleration or deceleration of spontaneous diastolic depolarization, fluctuations in the excitation threshold and resting potential, as well as with trace subthreshold and suprathreshold oscillations.
The mechanism of re-entry of excitation (re-entry) consists in repeated or multiple excitation of a section of the myocardium by the same pulse, making a circular motion. To implement this mechanism, two conduction pathways are required, and one of them impairs the passage of the impulse due to local unidirectional blockade.
 The area of the myocardium, to which the next impulse did not reach in a timely manner, is excited in a roundabout way with some delay and becomes a source of extraordinary excitation. It spreads to neighboring areas of the myocardium, if these areas have managed to get out of the state of refractoriness.
The area of the myocardium, to which the next impulse did not reach in a timely manner, is excited in a roundabout way with some delay and becomes a source of extraordinary excitation. It spreads to neighboring areas of the myocardium, if these areas have managed to get out of the state of refractoriness.
The macro re-entry mechanism is possible due to the functional division of the atrioventricular node into two parts, conducting impulses at different speeds due to functioning additional pathways (with WPW syndrome), and the micro re-entry mechanism is realized mainly by anastomoses in the branches of the conducting system.
Violation of impulse conduction is primarily due to a decrease in the action potential, which may be associated with a decrease in the resting potential. Conduction disturbances can develop due to a prolongation of the refractoriness period (slow repolarization) in the areas of the conduction system.
One of the mechanisms of conduction disturbance is the so-called decremental conduction, which consists in a progressive decrease in the rate of depolarization and action potential during the propagation of an impulse from one fiber to another. An important role in the mechanism of parasystolic arrhythmias is played by the so-called blockade of entry and exit in the region of the ectopic focus.
Under the blockade of the entrance is understood the impossibility of penetration into the ectopic focus of impulses of the main rhythm, and under the blockade of the exit- the impossibility of leaving this focus of part of the ectopic impulses.
The development of combined arrhythmias may be based on a combination of the above and some other mechanisms.
"Practical electrocardiography", V.L. Doshchitsin
Cardiac arrhythmias are one of the most common manifestations of cardiovascular diseases. In recent years, significant progress has been made in the diagnosis of rhythm and conduction disorders due to the use of new methods of long-term ECG recording, electrohysography, and programmed cardiac stimulation. These methods obtained new data on the anatomy and electrophysiology of the conduction system of the heart, on the pathogenetic mechanisms of rhythm and conduction disturbances. As a result…
I. Impulse formation disorders: sinus tachycardia. sinus bradycardia. sinus arrhythmia. migration of the rhythm source. extrasystoles: supraventricular and ventricular; single, group, allorhythmic; early, middle and late; paroxysmal tachycardia: supraventricular and ventricular; according to the re-entry mechanism and ectopic; non-paroxysmal tachycardia and accelerated ectopic rhythms: supraventricular and ventricular; according to the re-entry mechanism, parasystolic and elusive; atrial flutter: paroxysmal and persistent; right...
If in the process of deciphering the ECG, signs of any rhythm or conduction disturbance are detected, then a special technique should be used. Analysis of arrhythmia should begin with the identification of P waves, their regularity and atrial rate, which is determined in the same way as the ventricular rate. At the same time, changes in the atrial rate can be detected: its slowdown (sinus bradycardia, sinoauricular ...
You should proceed to the analysis of the ventricular rhythm: its frequency (if it was not previously determined) and the regularity of the R-R intervals. There may be individual premature QRS complexes against the background of the correct rhythm (extrasystoles), individual prolapse of ventricular complexes due to sinoauricular or atrioventricular blockade, or completely irregular, erratic rhythm characteristic of atrial fibrillation. It is also necessary to determine the width of the QRS complexes, the position of the electrical ...
If you have played a poker tournament at least once in your life, then you have probably come across such a concept as “re-entry”. Moreover, it exists both in online poker and in live tournaments, and it is used quite often. So what is re-entry in poker? What is it for, and should it be used during the tournament? Let's figure it out...
Definition of the term
Re-entry in poker (English “re-entry” - “re-entry”)- this is the player's ability to make an additional rebuy of chips in the event that he loses his entire initial stack. In fact, this term means the same as. But is it really useful to buy additional chips in a tournament? Or is it better to get up and leave the tournament, if today is not lucky?
In fact, poker re-entries are useful for tournaments for two reasons:
- The prize fund of the tournament is accelerating.
- The chances of professionals to succeed are increasing.
Let's take a closer look at each of these reasons.

Prize fund growth
Of course, if players can buy more chips every time they lose their stack, then the prize pool of the tournament will slowly but surely grow, which means that the interest of other participants in this tournament will also increase. And, interestingly, as the prizes in the tournament increase, the number of players who made an additional purchase also increases.
The logic here is quite simple. Players see the tournament's prize pool grow, and even if they lose their starting stack, they try again by re-entry and buying more chips. Moreover, in modern tournaments, an unlimited number of rebuys is most often introduced, which means that you can rebuy chips again and again, accelerating the prize pool of the tournament.
Increasing the chances of professionals
Today, even novice poker players know that absolutely any hand can win the hand. You can go all-in with two aces and end up losing to the person holding 7-2 offsuit. And it happens a lot more often than you might think. And that's why re-entry in poker allows you to increase the chances of professional strategists, and reduce the chances of lucky beginners, because luck cannot smile on them forever.
Accordingly, the mathematical expectation between the novice player and the regular, who acts according to a previously developed strategy, grows.

What's in practice?
However, everything that we have said above concerns only theory. In practice, things are somewhat different. After all, it is human to err, and even experienced players can sometimes begin to look for the reasons for their failures in themselves, even if they lost purely by chance. Therefore, we do not recommend re-entrying more than twice in the same tournament. Because the more “repurchases” you make, the greater your desire to “recoup” will be. Accordingly, you yourself will start to tilt, which in the end will not bring anything good for your bankroll.
On the other hand, the size of the rebuy is always the same, and usually it is equal to the size of the player's starting stack at the start of the tournament. That is, if at the very beginning of the tournament each of the players received a thousand chips, then for an additional purchase you will also receive a thousand game chips. However, it should be understood that at the beginning of the tournament the blinds were much smaller, and the stacks of the players were approximately the same.
And if you rebuy in the middle of a tournament, your 1,000 chips will be worth at most a few big blinds, while your opponents will have stacks of several tens of thousands of chips. Accordingly, you are unlikely to be able to successfully perform with such a limited stack.
Fortunately, re-entry in poker is possible only up to a certain period, after which the game “on the fly” begins.
The following factors lead to a violation of the conduction of an impulse in the heart:
1. Reducing the magnitude of action potentials.
2. Slowing down the propagation of the generated impulse to unexcited cells (for example, during the transition of the excitation wave from viable Purkinje fibers to dead working cardiomyocytes during myocardial infarction).
3. Violation of intercellular electrotonic interactions.
4. An increase in resistance to axial current from gap junctions as a result of an increase in the intracellular content of Ca 2+ ions (with myocardial ischemia or an overdose of cardiac glycosides).
5. Increased severity of myocardial anisotropy. Anisotropy is a property of the heart tissue to conduct an impulse differently depending on the direction of its movement. An increase in the severity of myocardial anisotropy is observed with the growth of connective tissue in the heart, as well as violations of the electrophysiological properties of the cells of the conduction system of the heart and working cardiomyocytes.
The manifestations of conduction disturbances are bradyarrhythmias or tachyarrhythmias. Bradyarrhythmias are more often observed with various heart blocks. Tachyarrhythmias are the result of (1) the appearance of accelerated escape rhythms against the background of a slowdown in the sinus node, (2) re-entry of the excitation wave - re-entry.
Pathogenesis of arrhythmias due to re-entry
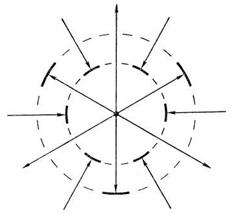
Under physiological conditions, after the generation of an impulse by the cells of the sinus node, the excitation wave propagates along the conduction system of the heart with a damped decrement. However, there are situations when the excitation wave does not die out, but recirculates, causing excitation of the myocardium. Arrhythmias, which are based on the recirculation of excitation, are caused by the re-entry mechanism - "re-entry" (English, Fig. 5). For re-entry to occur, the following conditions must be met:
Rice. 5 Schematic representation of the conditions necessary for the occurrencere- entry.
The substrate for re-entry can be almost any part of the heart. There are two types of re-entry - anatomical and functional. Anatomical re-entry is formed by morphological structures - for example, a loop of Purkinje fibers, accessory pathways, etc. Functional re-entry is much more common than anatomical and is formed by heart tissues with different electrophysiological properties. Alternative paths should have slower impulse conduction. A unidirectional impulse conduction block is observed if the impulse cannot propagate in one direction - for example, antegrade, but is able to propagate in the other direction - retrograde. This is explained by the fact that the cardiomyocytes that make up the circulation trajectory of the repeated excitation wave have different effective refractory periods. An impulse, which for some reason cannot propagate antegrade, goes by a roundabout, retrograde path. During this time, the effective refractory period of the area with a unidirectional block ends, and the excitation wave again reaches the area of the myocardium with increased automatism or trigger activity. The central zone of the impulse conduction block, around which the excitation wave circulates, is created by the anatomical features of the tissue, its functional properties, or combines these features.
It has been established that the mechanisms of excitation re-entry underlie many rhythm disorders: paroxysmal supraventricular tachycardia with re-entry of excitation in the AV node, paroxysmal tachycardia from the AV node, with tachyarrhythmias associated with the activation of congenital additional impulse conduction pathways (for example, Wolff-syndrome). Parkinson-White), atrial flutter and fibrillation, nodal rhythms from the AV junction, accelerated idioventricular rhythm, etc.
Classification of arrhythmias
ASSOCIATED WITH AUTOMATIC DISTURBANCES
A. Violations of the automatism of the sinus node
Sinus tachycardia
Sinus bradycardia
sinus arrhythmia
Sick sinus syndrome
B. Ectopic rhythms (heterotopic arrhythmias)
atrial rhythm
Nodal (atrioventricular) rhythm
Idioventricular (ventricular) rhythm
Migration of the supraventricular pacemaker
Atrioventricular dissociation
RELATED TO EXCITABILITY DISTURBANCES
Extrasystole
Paroxysmal tachycardia
ASSOCIATED WITH IMPAIRMENT OF EXCITABILITY AND CONDUCTIVITY
Atrial fibrillation (fibrillation) (atrial fibrillation)
atrial flutter
Flutter and fibrillation (flicker) of the ventricles
CONDUCTIVITY RELATED
Sinoatrial blockade
Intra-atrial block
Atrioventricular block
Intraventricular blockade (blockade of the branches of the bundle of His).
Syndromes of premature excitation of the ventricles
a) Wolf-Parkinson-White syndrome (WPW).
b) Syndrome of the shortened PQ interval (CLC).
the occurrence of arrhythmia according to the mechanism: early and late postdepolarization, macro- and micro-re-entry.
1) EARLY POST-DEPOLARIZATION- this is a premature depolarization of myocardial cells and the conduction system, which appears when the repolarization phase of the action potential has not yet been completed, the membrane potential has not yet reached the resting potential. This premature AP is considered to be triggered (induced) because it owes its onset to early post-depolarization emanating from the main AP. In turn, the second (induced) AP, due to its early post-depolarization, can cause a third, also trigger AP, and the third AP - the fourth trigger AP, etc. If the source of trigger activity is in the ventricles, then on the ECG a similar type of disturbance in the formation of impulses manifests itself as ventricular extrasystole or polymorphic ventricular tachycardia.
You can specify two of the most important conditions for the occurrence of early post-depolarizations, such as: prolongation of the repolarization phase of the action potential and bradycardia. With a slowdown in repolarization and, accordingly, an increase in the total duration of AP, premature spontaneous depolarization may occur at a time when the repolarization process has not yet been completed. With a decrease in the frequency of the main heart rhythm (bradycardia), there is a gradual increase in the amplitude of early postdepolarizations. Having reached the threshold of excitation, one of them causes the formation of a new AP even before the completion of the original one.
Since early post-depolarizations are realized due to the activation of Na+- and Ca2+-channels, it is possible to suppress associated cardiac arrhythmias with the help of blockers of these channels.
The occurrence of early post-depolarizations is facilitated by: hypercatecholaminemia, hypokalemia, acidosis, ischemia, long QT syndrome. Often, such automatism is the result of the use of antiarrhythmic drugs that block K + channels (sotalol, quinidine, etc.).
2) LATE (DELAYED) POST-DEPOLARIZATIONS- this is a premature depolarization of myocardial cells and conductive tissue, which appears immediately after the completion of the repolarization phase. Occur, as a rule, after partial hyperpolarization (trace potentials). If the post-depolarization amplitude reaches the AUD, AP occurs, etc. Subthreshold fluctuations in the membrane potential, which can normally be present, but never manifest themselves, under pathological conditions that cause Ca2+ overload of cardiomyocytes, can increase in amplitude, reaching the threshold of excitation.
An increase in the intracellular concentration of calcium ions causes the activation of non-selective ion channels, which provide an increased supply of cations from the extracellular environment to the cardiomyocyte. At the same time, mainly Na+ ions enter the cell, the concentration of which in the extracellular fluid is much higher than the level of K+ and Ca2+. As a result, the negative charge of the inner surface of the cell membrane decreases, reaching a threshold value, followed by a series of premature APs. Ultimately, a chain of trigger excitations is formed.
Trigger activity of heart cells associated with delayed post-depolarizations can occur under the action of cardiac glycosides or catecholamines. Very often it appears with myocardial infarction.
3)For the formation of MACRO RE-ENTRY with its characteristic properties, certain conditions are required:
The presence of a stable closed loop, its length depends on the anatomical perimeter of the non-excitable obstacle around which the impulse moves;
Unidirectional blockade of conduction in one of the segments of the re-entry loop;
The duration of the propagation of the excitation wave must be shorter than the time during which the impulse can travel the entire length of the re-entry loop. Due to this, in front of the front of the pulse propagating in a circle, there is a tissue section that has left the state of refractoriness and has managed to restore its excitability (“window of excitability”).
The mechanism of macro reentry is believed to underlie atrial flutter.
This circulation can be eliminated by lengthening the refractory period. In this case, the “window of excitability” may close, since the circulating wave encounters a region that is in a state of refractoriness. This can be achieved with the help of antiarrhythmic drugs that block K + channels, which leads to a slowdown in repolarization and an increase in the duration of the refractory period. In this case, the "window of excitability" closes, and the movement of the impulse stops.
4) With MICRO RE-ENTRY the movement of the impulse occurs along a small closed ring, not associated with any anatomical obstacle. The impulse makes not only circular, but also centripetal motion. Closer to the center, AP decreases, and excitation fades, cells in the center give only a local response, because are in a state of refractoriness and, as it were, replace an anatomical obstacle.
Apparently, many complex tachyarrhythmias, in particular fibrillations, are associated with the micro re-entry mechanism. Combinations of loops lying in different planes occur in patients with ventricular tachycardia in the acute period of myocardial infarction.
Very often, the morphological substrate for the occurrence of re-entry is the Purkinje fibers located in the ischemic zone. These cells are resistant to hypoxia and may not die in the focus of infarction. However, at the same time, they change their electrophysiological characteristics in such a way that fast Na+ channels turn into “slow” ones. In this case, the conduction of the impulse slows down and it leaves the ischemia zone at the moment when the rest of the myocardium is already in a state of relative refractoriness and is ready for re-excitation, but the impulse from the sinus node has not yet arrived. The re-entry phenomenon occurs when the myocardium is stimulated twice by the same impulse: the first time when it enters from the sinus node, and the second time when it re-enters the ischemic zone. In this case, it is possible to break the re-entry loop with the help of drugs that block "slow" Na + channels in the ischemic zone (lidocaine, novocainamide).
The undoubted advantage of these antiarrhythmics is that they show a high affinity specifically for abnormal Na+ channels in the ischemic zone and practically do not inhibit fast Na+ channels in healthy myocardial cells, and therefore do not affect electrophysiological processes in intact cardiomyocytes.